By marko_laaksomaa  -
-
- Mon Nov 04, 2019 9:14 am
#755
Hi
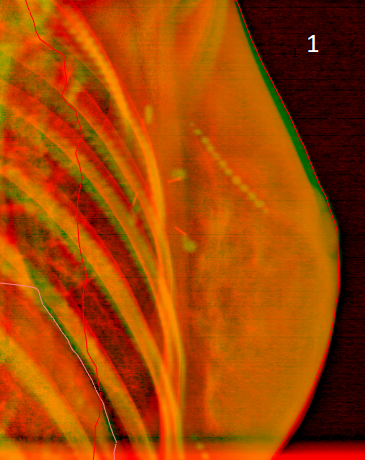
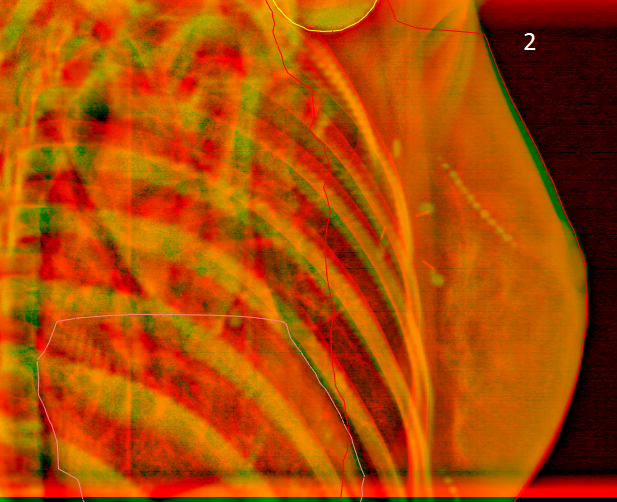
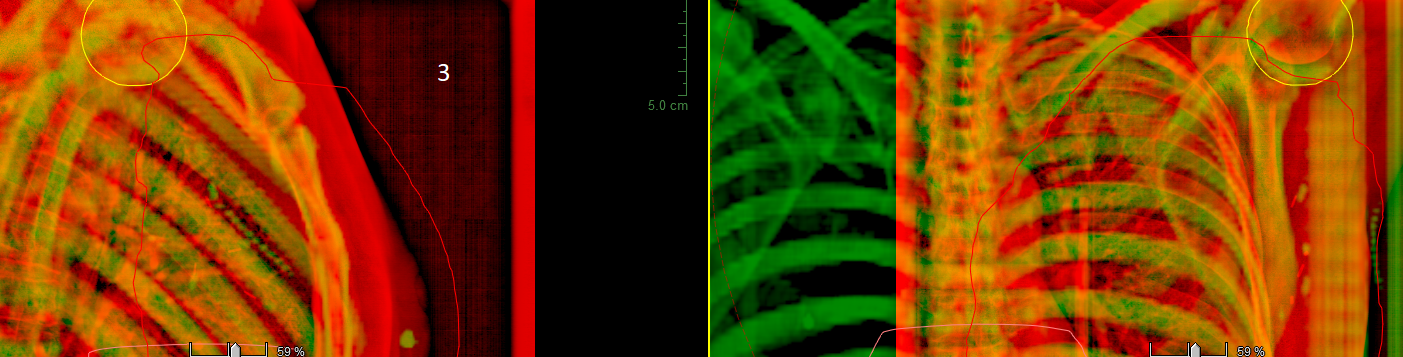
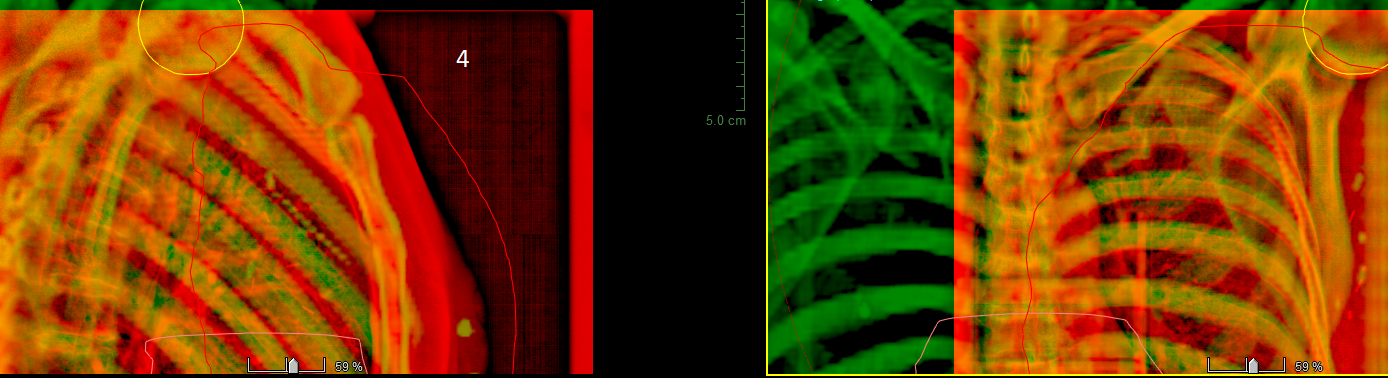
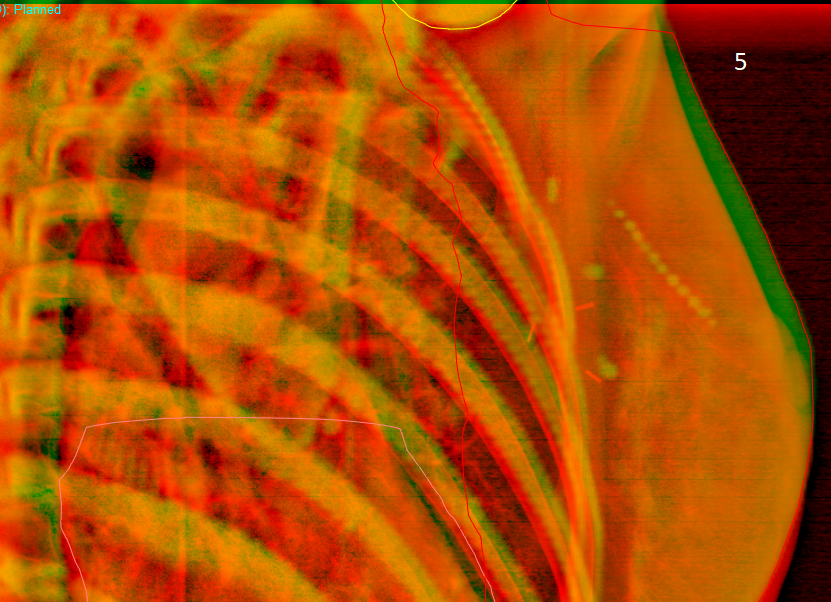
At the moment we acquire daily tangential and weekly additional AP+LAT images in DIBH n+ and mastectomy cases with AlignRT, usually there is no surprises due to exceeding of IGRT tolerances in the weekly AP+LAT images and we can mostly continue with tangential images for a week. In tangential images we have (together with ribs+ breast) also vertebra and shoulder joint daily visible so we can approximately daily evaluate the accuracy for the lymph node area and BHL. In those images pretty typical situation seems to be such that there is -0.1 - -0.4 cm couch shift needed for the vertebra in LNG (vertebra locates too cranial in the first place in comparison to reference image), but ribs LNG is ok and thereby there is no need to apply the couch shifts. At the treatment, some of those patients takes BH in the latest treatment fields some mm too much towards cranial direction in LNG based on AlignRT deltas, and based on findings earlier in the published study with RPM. As a conclusion based on findings in practice, for some DIBH patients there are situations in practice that we should leave BH LNG delta 1-3 mm too caudally from zero at the BH setup to optimize the treatment accuracy (then also vertebra LNG would be in correct location in the first place) and to eliminate the risk that patient exceeds the LNG threshold (4 mm) with taking the BHs too cranial at the end of the fraction. The reason for this may be that the patient has possibly taken 3-5 BHs more at the CT just before CT was acquired than she takes at the setup process. Therefore at the setup we can not copy that "pitch" which appears only after patient has taken several BHs. The other reason (for other patients) for the vertebra displacement in LNG may be that BHL in the images is 1-3 mm too shallow in the first place, when vertebra in LNG usually remains at least as much too cranial in the images, but that is another story already. One thing that I have noticed is that if we leave 1° roll and 2 mm LAT error to the "same" direction at the BH setup with AlignRT, there can be 5 mm displacement in the images in LAT. These are such some may think insignificant things that may be workflow related issues and things that you do not have, but I tried to bring something to think about here to the forum again from the practice.
Have a nice week
Marko
At the moment we acquire daily tangential and weekly additional AP+LAT images in DIBH n+ and mastectomy cases with AlignRT, usually there is no surprises due to exceeding of IGRT tolerances in the weekly AP+LAT images and we can mostly continue with tangential images for a week. In tangential images we have (together with ribs+ breast) also vertebra and shoulder joint daily visible so we can approximately daily evaluate the accuracy for the lymph node area and BHL. In those images pretty typical situation seems to be such that there is -0.1 - -0.4 cm couch shift needed for the vertebra in LNG (vertebra locates too cranial in the first place in comparison to reference image), but ribs LNG is ok and thereby there is no need to apply the couch shifts. At the treatment, some of those patients takes BH in the latest treatment fields some mm too much towards cranial direction in LNG based on AlignRT deltas, and based on findings earlier in the published study with RPM. As a conclusion based on findings in practice, for some DIBH patients there are situations in practice that we should leave BH LNG delta 1-3 mm too caudally from zero at the BH setup to optimize the treatment accuracy (then also vertebra LNG would be in correct location in the first place) and to eliminate the risk that patient exceeds the LNG threshold (4 mm) with taking the BHs too cranial at the end of the fraction. The reason for this may be that the patient has possibly taken 3-5 BHs more at the CT just before CT was acquired than she takes at the setup process. Therefore at the setup we can not copy that "pitch" which appears only after patient has taken several BHs. The other reason (for other patients) for the vertebra displacement in LNG may be that BHL in the images is 1-3 mm too shallow in the first place, when vertebra in LNG usually remains at least as much too cranial in the images, but that is another story already. One thing that I have noticed is that if we leave 1° roll and 2 mm LAT error to the "same" direction at the BH setup with AlignRT, there can be 5 mm displacement in the images in LAT. These are such some may think insignificant things that may be workflow related issues and things that you do not have, but I tried to bring something to think about here to the forum again from the practice.
Have a nice week
Marko